





- The condition most commonly occurs at puberty (physiological gynaecomastia), it may resolve by the time individuals reach their twenties, but often it fails to.
- The condition may be related to being overweight
- Drugs such as hair growth promoters or body building drugs can cause gynaecomastia (iatrogenic)
- Occasionally the condition may be related to a hormone imbalance.
- Very rarely it may be related to a breast cancer (especially if the patient has a mutation on the BRCA gene)
The severity is determined in terms of the excess volume and excess skin.
Grade 1= Mild enlargement with no excess skin
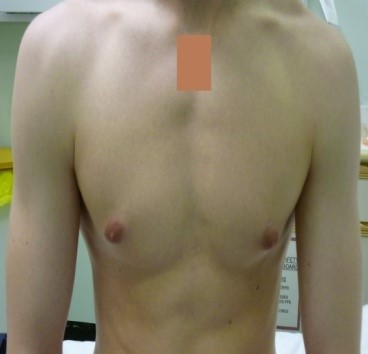
Pre-op

39gm Gland

16 months post-op
Grade 2a/b= Moderate enlargement with or without excess skin

Pre-op

178gm Gland

1 year post-op
Grade 3= Large enlargement with excess skin
Pre-op

246gm Gland

17 months post-op
Different techniques exist for removal of Gynaecomastia and what follows is my personal view based on my research, experience and learning.
- Trans-axillary removal of gynaecomastia; tissue (Levick/Vijh technique). This technique involves removal of effectively all of the gynaecomastia tissue through a 2cm incision in the armpit (this technique was used on all of the patients shown above). It gives a result that leaves no obviously visible scar, as this is almost impossible to perceive as it is so small and is in the armpit. For more information visit our male plastic surgery site manoftomorrow.com
- Removal of gynaecomastia through an incision around the areolar. This leaves a scar in a prominent position on the chest and runs the risk of taking away one thing you are embarrassed about and replacing it with another.
- Liposuction; this technique can be useful where the main problem is one of excess fat tissue, and the patient does not want to remove all of the gynaecomastia tissue. In my opinion it is of little use in a slim patient, whose gynaecomastia is largely glandular as in the grade 1 patient shown above (ie there is no fat to liposuck). I also believe that in patients where the majority of the problem is glandular, this can make the situation worse. This is because breast/gland tissue is a modified sweat gland ie it is derived from and attached to skin, thus when liposuction is carried out the gland which is attached to the skin may sag even more after the liposuction than it did before.
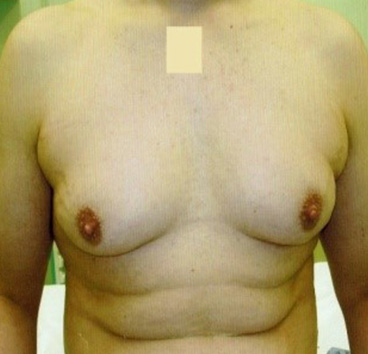
- Mastectomy and adjustment of the nipple position. Where the excess skin is so great that it is unlikely it will re-drape and we believe that the patient will be left with large volumes of sagging skin, one can excise the skin and gland tissue and then replace the nipple at a higher position. This leaves obvious scarring on the chest. As in the picture below
Mastectomy and Free nipple graft

Before


After

For further advice, feel free to contact us by phone on 0121 794 2369
Before and After



Fee Range
Gynaecomastia (man boobs)
Starting at £7395